Chest Pain EMR Documentation Workflow: ICD-10-CM, Cardiology Notes, and Triage Context
Official Source Basis
- Chest pain category: The April 1, 2026 ICD-10-CM tabular file lists R07 as Pain in throat and chest.
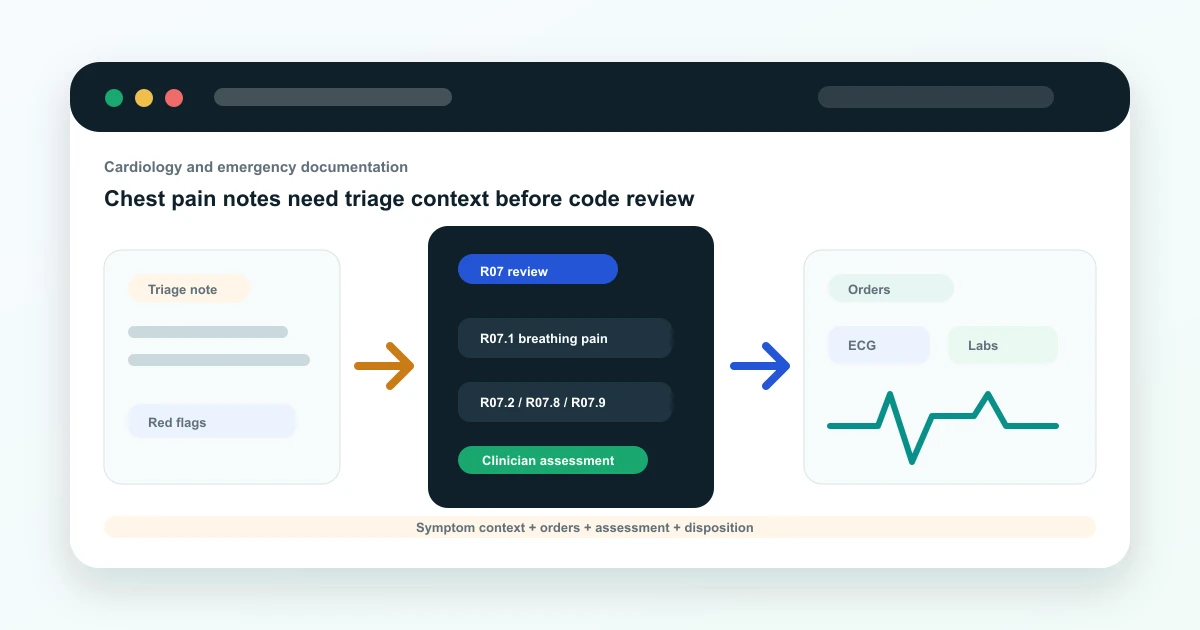
- Subcategories: R07 includes entries such as R07.1 chest pain on breathing, R07.2 precordial pain, R07.8 other chest pain, and R07.9 chest pain, unspecified.
- Exclusion context: The R07 category includes Excludes notes, which is why symptom coding needs official-source review.
Chest pain documentation starts with triage context
Chest pain is not just a diagnosis field. In an EMR, it is a triage and documentation workflow that may include onset, character, radiation, vitals, risk factors, ECG, lab orders, doctor assessment, disposition, and follow-up.
The EMR should help teams capture symptom context without implying that software diagnoses the patient.
ICD-10-CM R07 source context
Source note: this article uses the CDC/NCHS ICD-10-CM Tabular List, Index, and April 1, 2026 update files as the coding source. It is written for EMR workflow education, not as a substitute for official coding review.
The official tabular file places chest pain concepts under R07, Pain in throat and chest. The subcategories include chest pain on breathing, precordial pain, other chest pain, and unspecified chest pain.
That structure is useful for EMR design because it reminds teams that symptom documentation needs context and clinician assessment before final code selection.
- R07: pain in throat and chest.
- R07.1: chest pain on breathing.
- R07.2: precordial pain.
- R07.8 and R07.9: other or unspecified chest pain contexts.
What the EMR should capture
A chest pain workflow should capture symptom narrative, red flags, vitals, risk factors, orders, clinician assessment, and disposition. This is especially important in hospital, emergency, and cardiology workflows where the care path may move quickly.
- Onset, character, radiation, and associated symptoms.
- Vitals and red-flag context.
- ECG, lab, imaging, or referral orders when used.
- Clinician assessment and disposition.
- Follow-up plan or escalation record.
Where AI can help
AI can summarize the symptom narrative, structure the visit note, and identify missing documentation fields such as onset or disposition. It can also surface R07-related candidates for review when the note is symptom-focused.
Where doctor and coder review is required
The final clinical assessment, diagnosis, disposition, and code selection require qualified review. AI suggestions should remain draft support, especially for high-risk symptoms.
This article is educational and does not replace certified medical coding guidance. Final code selection should be reviewed by qualified clinical or coding staff using the official ICD-10-CM guidelines for the correct date of service.
How Vivalyn EMR supports chest pain workflows
Vivalyn EMR connects triage-style documentation, Patient 360, orders, AI-assisted notes, billing, and department workflows so cardiology and hospital teams can preserve context from first complaint through follow-up.
Want to turn source-backed clinical documentation into an operational EMR workflow? Vivalyn EMR connects AI-assisted notes, doctor review, Patient 360, billing, analytics, and department workflows in one platform.
Continue From Coding Education to EMR Evaluation
Use this guide with the Vivalyn EMR feature set, department workflows, billing pages, and demo path.
Vivalyn EMR Hub
Start with the core AI EMR product page for clinics and hospitals.
Next pathEMR Features
Review OPD, IPD, Patient 360, billing, lab, pharmacy, and AI workflows.
Next pathEMR Software India
Commercial product page for ABDM-ready EMR software in India.
Next pathClinic Management Software
Evaluate front desk, appointments, billing, inventory, and self check-in.
Next pathEMR by Department
Find specialty and hospital department workflows mapped to EMR use cases.
Next pathPatient Experience
Review patient self check-in, reminders, engagement, and front-desk flow.
Next pathCompliance & Security
Evaluate privacy, access controls, audit trails, and deployment governance.
Next pathEMR by Country
Browse international EMR software pages by country and deployment context.
Next pathEMR by City
Explore city-specific EMR pages for Hyderabad, Bengaluru, Mumbai, and Delhi.
Next pathEMR Alternatives
Compare Vivalyn EMR with common clinic and hospital software alternatives.
Next path2026 EMR Burden Dataset
Use the benchmark dataset on Indian EMR adoption and documentation burden.
Next pathStart 30-Day Free Trial
Move from research to product walkthrough, trial, and implementation planning.
Next pathEMR Knowledge Hub
Read implementation, migration, ABDM, and hospital workflow guides.